
14 red flags that can disqualify a dental practice. From low new patient counts to fee-for-service risk, learn what to watch for before you commit.
I've looked at over 500 practices. Most of them I tell my clients to walk away from. That's not pessimism. That's just reality. Not every practice is a good acquisition. You need to know what to look for.
Here are the 14 red flags I watch for. When I see one of these, alarm bells go off. When I see two or three, the practice goes on the "no" pile. These are things that either indicate deeper problems or will cost you significantly down the road.
1. Low New Patient Count
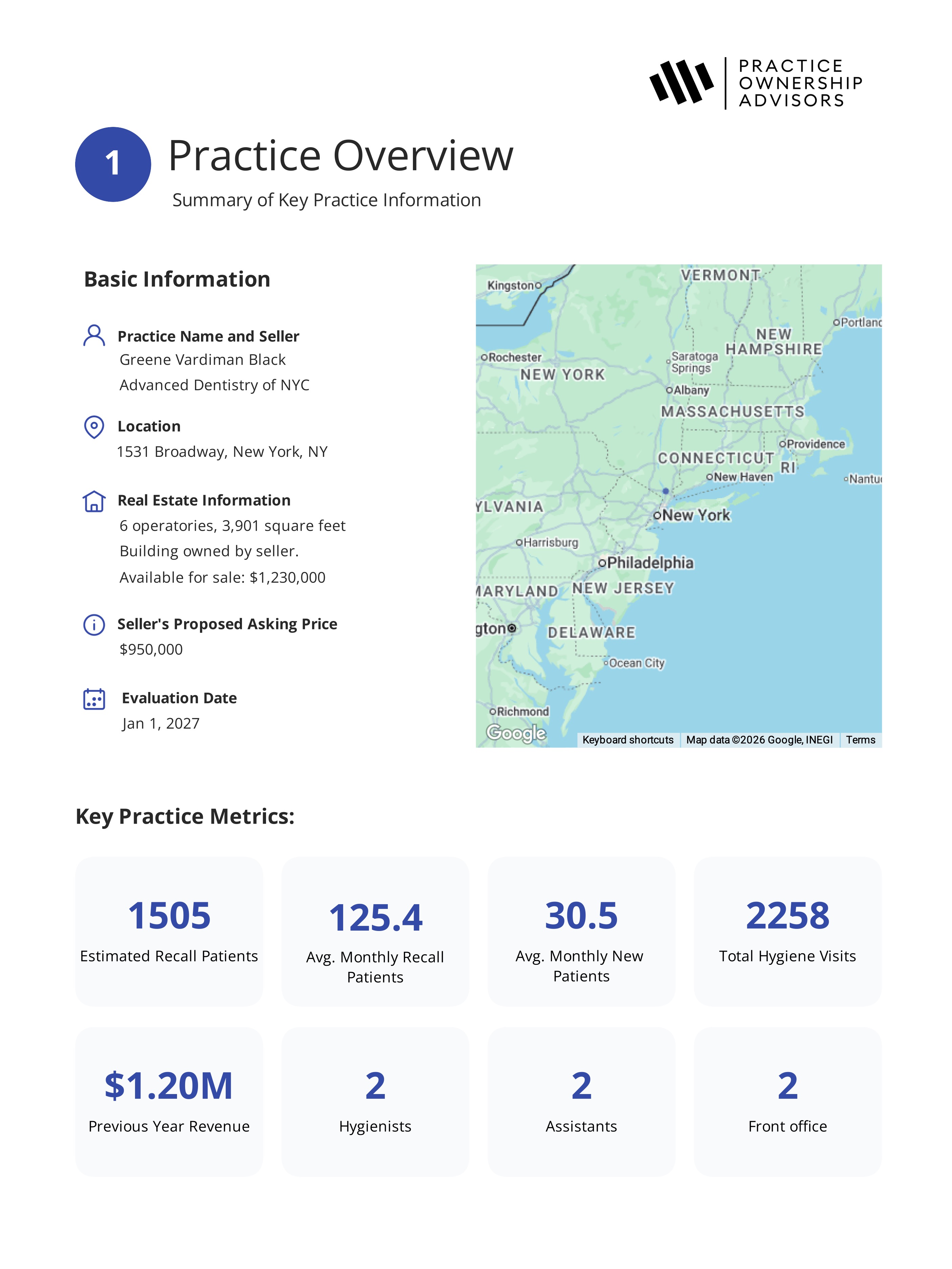
A healthy practice is constantly bringing in new patients. I want to see at least 150-200 new patients per year, depending on the practice size. If a practice is only getting 50 new patients a year, that could be an indication that the practice is in a saturated area or a bad location.
Here's something important about acquisitions versus startups. When you're doing a startup, you're relying on demographic studies and theories about how many patients you might attract. When you're buying an existing practice, you can look at the previous dentist's actual new patient numbers to see how the demographics play out in reality. You're not guessing. You're seeing the results.
If the practice isn't getting many new patients, something is broken. Depending on the situation, it might be something you can fix, like marketing or hours, or it might be something inherently bad about the practice's location that you can't change.
However, sometimes low new patient numbers actually represent a growth opportunity. I've worked with clients who purchased practices where the previous dentist was literally turning away new patients because they didn't have the capacity to see them. If you go in and add availability, you can open the floodgates and grow the practice significantly.
2. Low Active Recall
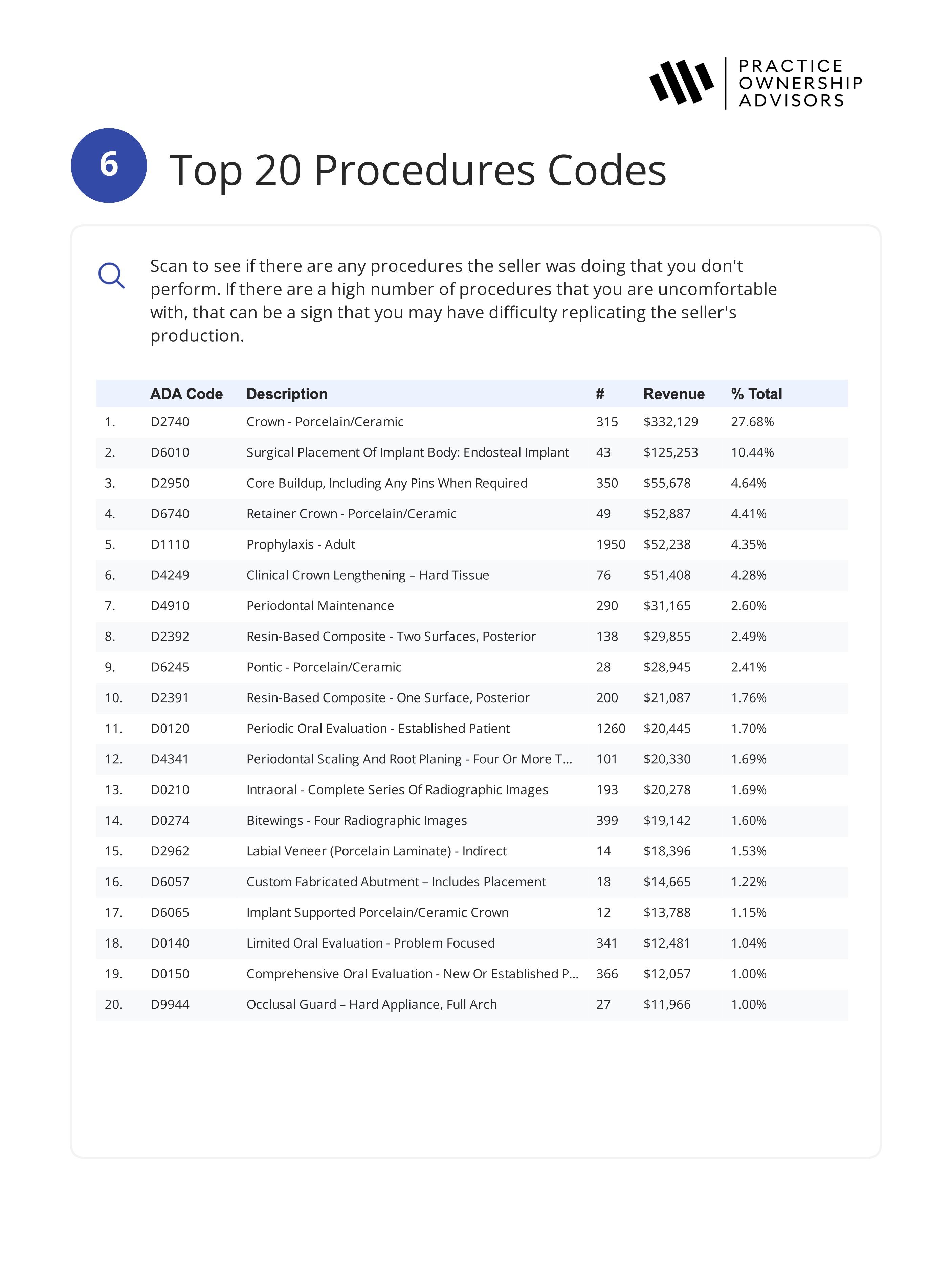
A low number of active recall patients is one of the biggest red flags I look for. You can estimate active recall by taking the number of periodic exams (D0120) and dividing by about 1.5. For a healthy solo practice, I want to see at least 1,200 to 2,000 active recall patients.
This is how you make your money as a practice owner. Recall patients come in for their cleanings and exams, and that's where your treatment plans come from. They need crowns, fillings, perio treatment, implants. If you don't have enough patients coming through the door, you don't have enough opportunities to produce. It's that simple.
If the recall count is well below 1,000, you either have a patient retention problem or the practice is just too small to support your financial goals.
3. Poor Insurance Mix
Ask about the insurance breakdown. Are 80% of patients on Medicaid or HMO plans? What's the mix of PPO, self-pay, and fee-for-service?
Heavily Medicaid or HMO-dependent practices have lower profit margins and higher administrative burden. A healthy PPO-based mix with some cash patients is generally what you want to see. A mixed panel gives you reasonable reimbursement and predictable revenue.
4. High Production Per Patient
If the average patient is generating $1,000+ per year in production, something might be off. That may signal aggressive treatment planning, overtreatment, or a clinical approach that won't transfer to you as the new owner.
Why it matters: above-average production per patient often doesn't stick around under new ownership. If the seller's clinical philosophy drove those numbers, your baseline revenue could drop significantly once you take over.
5. High Rent
Most overhead items you can change as the new owner. You can adjust staffing, renegotiate supply contracts, and change how you run the business. But rent is difficult to change, especially if the seller locked into a long-term lease or if the landlord isn't willing to negotiate.
If the practice is paying an outsized percentage of revenue in rent, that's a structural problem that eats into your profit every single month and limits what you can take home.
6. Seller Not Fully Retiring
Ideally, the dentist selling the practice is fully retiring. When patients find out their dentist is retiring, they accept the transition. They understand the practice is under new ownership and they give you a chance.
But if patients find out the seller is just working at a new office down the road, many of them are going to follow the seller. They've been seeing that dentist for years, maybe decades. Given the choice between a familiar face somewhere else and a stranger in the same building, a lot of patients will choose the familiar face.
One way to check this is to ask the seller directly what their plans are after the sale. If they're planning on moving out of the area, that's great. If they're younger and staying local, that's a much higher red flag, because there's a good chance they'll start practicing again, and your patients will have the option to follow them.
7. Seller Owns Multiple Practices
Walk carefully here. Why are they selling this one? Are they consolidating? Are they dumping a bad location? Did they overexpand and now they're in trouble? What's the real story?
Why it matters: sellers with multiple practices often have complicated motivations. They might be selling the one that's failing while keeping the one that works. You need to understand why this specific practice is for sale.
8. Staff Are Mostly Family of the Seller
If the seller's spouse is the office manager, their daughter is the dental assistant, and their nephew works the front desk, you need to plan for the very real possibility that most of those people are going to leave when the seller leaves.
Why it matters: family members of the seller are there because of the seller, not because of the practice. When ownership changes, they often don't stick around. And replacing an office manager, a hygienist, or key support staff all at once is extremely difficult. You're essentially rebuilding the team from scratch while also trying to learn the practice and retain patients.
9. Key Staff Nearing Retirement
Who's the hygienist? How old are they? What about the office manager or the lead assistant? If your key producers are 5-10 years from retirement, you're buying a depleting asset.
Why it matters: replacing experienced staff is expensive and time-consuming. You lose continuity and efficiency. If you can't replace them before they leave, your revenue takes a hit.
10. Declining Hygiene Department
Look at the last three years of hygiene production. Is it going up, flat, or down? Down is bad.
What often happens is that a hygienist leaves and the seller decides not to replace them. Patients who were scheduled with that hygienist don't get rescheduled, some of them drift away, and the active patient count drops. By the time you're looking at the practice, you've lost patients that you're never getting back.
Your hope when buying a practice is that patients are sticking around. A declining hygiene department tells you they're not, and that's a problem that directly impacts the patient base you're paying for.
11. Heavy Out-of-Network or Fee-for-Service Mix
A practice that operates mostly out of network or cash-only can look incredible on paper. The fees are higher, the margins are better, and the P&L looks beautiful. But there's a hidden risk.
Those patients are paying more than they'd pay at the practice across the street, and they know it. They stay because they've built a relationship with their dentist over 10 or 20 years. The seller has earned that relational capital over a long time.
When you buy the practice, you don't inherit that relational capital. You're a new face asking patients to keep paying premium prices. Some will stay and give you a chance, but many will start wondering why they're paying double when there's an in-network provider down the road.
That puts you in a tough spot. Do you lower your fee schedule? Do you start going in-network with insurance companies, which drops your fees across the board? Either way, the revenue you thought you were buying may not be the revenue you actually get.
I'm not saying don't buy a fee-for-service practice. But you have to be extra careful with how you plan the transition, because patient attrition can be significantly higher than with an in-network practice.
12. Sudden Revenue Spikes Before Sale
This is sneaky. A practice runs flat for three years, then suddenly in year four revenue jumps 25%. That's fishy. What changed? Did the seller add expensive elective cases that won't repeat? Did they push cosmetic work that new patients won't accept?
Why it matters: these spikes often don't stick around. You're getting excited about revenue that won't last past the first year. You're overpaying for a phantom number.
13. Young Seller with No Clear Exit Reason
A 35-year-old dentist selling a thriving practice without a clear reason is suspicious. Are they burned out? Did they make a mistake buying it? Is there something about the location or business they're not telling you?
Why it matters: the reasons dentists sell matter. A seller who's retiring at 65 is different from a seller who's bailing at 40 for mysterious reasons.
14. Inadequate Parking or Limited Operatories
Check the physical space. Is there enough parking for patients? Can you fit enough operatories to grow the practice, or are you maxed out on day one?
Why it matters: practices with poor parking see new patient no-shows. Limited operatory capacity means limited growth. These are permanent constraints that you can't fix.
What You Do With These Flags
Finding one red flag doesn't automatically disqualify a practice. Sometimes there's a good explanation. The hygienist is 60, but they love their job and plan to work another 10 years. The seller is staying in town, but they're moving to a different specialty. These things happen.
What matters is asking the questions and understanding the story behind the flag. When you see multiple red flags, or when the explanations don't satisfy you, that's when you walk away.
Remember: only 15-20% of practices are worth buying anyway. You've got optionality. You don't need this one. Patience in the search is patience that pays off when you actually buy.

Practice Evaluation & Advisory Service
Independent clinical and financial analysis to help you make an informed decision before you buy.
Learn more

Newsletter + Free Practice Evaluation Checklist
One actionable email per week on buying the right practice, plus an instant download of our free Practice Evaluation Checklist.
One email per week. Checklist delivered instantly. Unsubscribe anytime.